Refractive surgery
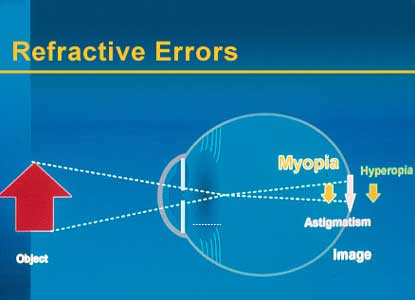
Spectacles or contact lenses compensate for refractive errors by altering the focus of light rays using negative (myopia), positive (hyperopia) or mixed (astigmatism) optical correction.
In myopia the eye is too long and the light rays are focused in front of the retina: long-distance vision is blurred. 25% of the adult population is short-sighted.
Hyperopia means the eye is too short and the light rays are focused behind the retina: near vision is blurred. Young patients do not realize this as their lenses are still supple and able to accommodate and compensate for hyperopia. The lens loses its elasticity with ageing and hyperopia gradually becomes apparent.
In astigmatism the curve of the cornea is not the same in every plane: instead of being round like a football it is flattened like a rugby ball. This causes image distortion, both in long-distance and near sight. Myopia and hyperopia are often associated with a degree of astigmatism.
At the age of 45 we all become presbyopic. This condition is caused by loss of lens elasticity and accommodation, which has to be compensated for by the wearing of reading glasses. Short-sighted presbyopics are often able to read without spectacles.
Refractive surgery as an answer
Spectacles or contact lenses compensate for refractive errors by altering the focus of light rays using negative (myopia), positive (hyperopia) or mixed (astigmatism) optical correction. The light rays are thus focused on the retina.
Advances in refractive surgery enable almost all refractive errors to be corrected with increasing predictability. These techniques - with the exception of phakic implants and clear lens extraction - alter eye focus by changing the curve of the cornea. In cases of myopia the optical zone (the centre) of the cornea is flattened to reduce its refractive power. In cases of hyperopia the cornea is curved to create extra refractive power. In cases of astigmatism the asymmetric shape of the cornea is modified in the axis of the astigmatism.
Spectacles and, more recently, contact lenses, have for long been the only means of correcting refractive errors in the human eye. Various refractive surgery procedures now open up new possibilities, not only for the myopic, but for astigmatic and hyperopic patients.
Many patients depend on spectacles or contact lenses, but ultimately find them uncomfortable or unattractive. In many cases, refractive surgery can reduce or eliminate such dependence.
Patient selection
Refractive surgery procedures would be a reliable alternative for all motivated and informed patients aged over 18 with more or less stabilized refraction.
Individuals satisfied with traditional correction will not necessarily be interested in surgery, while patients who have difficulty tolerating contact lenses or who have a profession or who practise a sport in which high visual acuity without correction is useful (e.g. firefighters) may request an operation.
It is best not to operate on patients who demand perfect results. The primary purpose of all refractive surgery is patient satisfaction, not necessarily 20/20 vision without correction. Prior to any operation an evaluation must be made with the patient to determine whether surgery will achieve the desired result. The patient must be told that all refractive surgery techniques may not be entirely precise and be informed of any risks or secondary effects and of the possible need for re-treatment. Some patients may still require correction in specific circumstances, e.g. for driving at night or reading film subtitles. As these techniques do not prevent presbyopia, slight under-correction of one eye may be considered in order to make reading easier, especially if the patient is over 40.
Conclusion
Today a wide range of surgical techniques is available to correct almost all refractive errors. They enable patients to become totally or largely independent of spectacles or contact lenses. Tens of thousands of patients have undergone these procedures, most of which involved no complications - to the great satisfaction of the patients.
All applicants for refractive surgery must be clear about the facts when making their informed decision; their hopes must be realistic and they must be aware of potential risks and complications.
The foregoing techniques may be applied as follows :
- Radial keratotomy: myopia up to -3 dioptres
- Astigmatic keratotomy: astigmatism up to 6 dioptres
- PRK with Excimer laser: myopia up to -5 dioptres, hyperopia up to +3 dioptres, astigmatism up to 3 dioptres
- LASIK: myopia up to -12 dioptres, hyperopia up to +6 dioptres, astigmatism up to 6 dioptres
- Phakic implants: myopia from -8 to -22 dioptres, hyperopia from +4 to +12 dioptres. Even higher refractive errors can also be corrected using a combination of phakic implants and LASIK (Bioptics).
- Clear lens extraction: myopia up to -30 dioptres, hyperopia up to +14 dioptres.
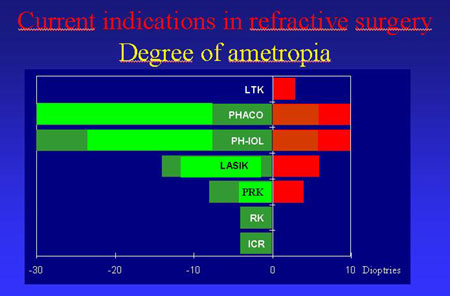
Holmium or Diode Laser Keratoplasty and Intra-corneal Rings are techniques that Dr. Vryghem does not perform and does not intend to perform.
Read more about refractive surgery in this brochure
If you want more information, or would like to make an appointment:
Contact us or call 0032 (0)2 741 69 99